Bleeding Changes the Whole Situation Fast
A lot of first aid problems give you a little time to think. Bleeding does not always offer that kindness.
When blood is really moving, the room seems to get smaller. People talk louder, hands get clumsy, and someone almost always wastes a few seconds doing the wrong gentle thing because they do not want to hurt the injured person. I understand that instinct. It is normal. It is also how manageable bleeding starts turning into a real emergency.
The first ugly truth is simple: if a person is bleeding heavily, comfort comes second for a while. Not forever. Just while you stop the leak.
That sounds harsh, maybe, but pressure has to be real pressure. A loose towel laid on top like a polite suggestion is not bleeding control. It is theater. Blood will go right through it, around it, under it. I have seen people keep lifting the cloth to check how things are going, and every time they do it they break whatever clotting was starting. They mean well. Means nothing. The body needs help, not curiosity.
What Actually Stops Bleeding
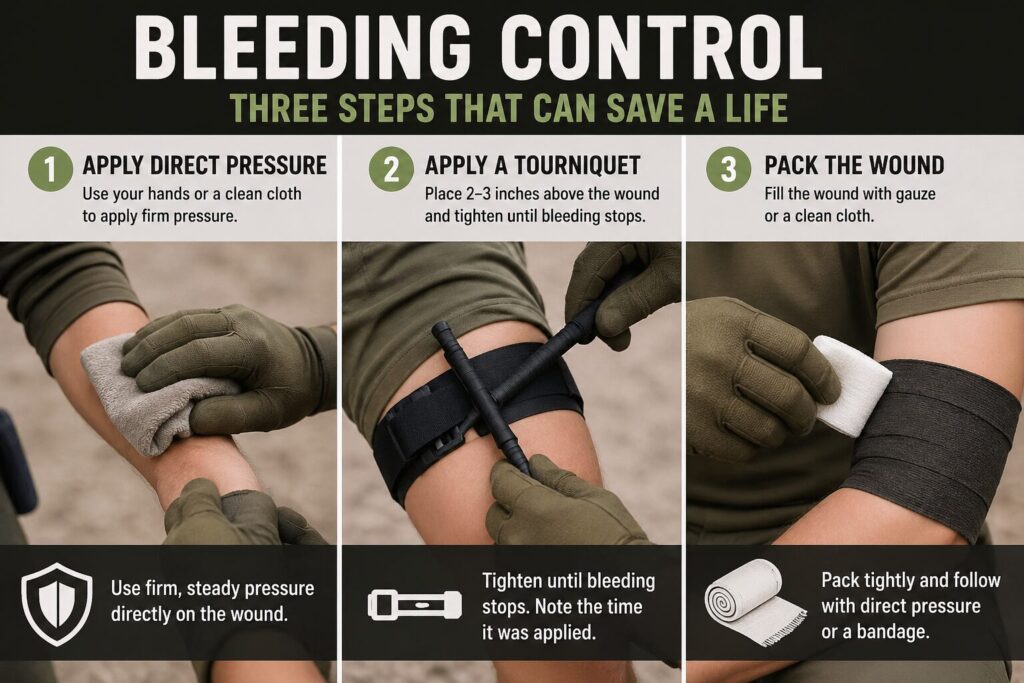
Most external bleeding control comes down to a short chain of actions: find the source, apply direct pressure, pack the wound if appropriate, and use a tourniquet when the bleeding is severe enough and the location makes that the right call. Not complicated on paper. In real life it feels messier.
Direct pressure works because blood vessels can sometimes be compressed enough that flow slows or stops, which gives clotting a chance to do its job. The body wants to solve the problem, but it needs time and a little force working in the same direction. That’s really the whole partnership.
The problem is that people often press too softly or give up too early. Heavy bleeding may require firm, sustained pressure with both hands and with most of your attention parked right there. This is not a light touch skill. If the person complains, that does not mean you are doing it wrong. Sometimes it means you are finally doing something that matters.
And yes, there is judgment in this. A scraped knee is one thing. Blood spurting, pooling quickly, soaking clothing, or continuing despite pressure is another thing entirely.
You Need to Look Past the Drama
Blood has a way of making everything feel worse than it is, but sometimes it also hides what is actually happening.
A scalp wound can look dramatic because the head bleeds a lot. A deep cut to an arm or leg can look oddly less theatrical at first and still be far more dangerous. So I do not like teaching people to respond to appearance alone. Respond to amount, speed, and location.
If blood is pulsing, pumping, or soaking through material quickly, assume seriousness. If the injured person is getting pale, weak, confused, sweaty, or strangely calm, assume blood loss is affecting the whole body now, not just the wound. That quiet, fading look some people get is not reassuring. It’s bad.
Now, before somebody turns this into a macho ritual, let me say the other half: you still work carefully. Gloves if you have them. Call emergency services early when the bleeding is significant. Keep yourself from becoming a second patient. There is no heroism in collapsing into the same mess.
Direct Pressure Done the Way It Actually Works
If I had to pick the one habit that saves the most fumbling, it would be this: once you identify the bleeding site, commit to pressure and stay there.
Use a clean cloth, dressing, gauze, or even clothing if that is what you have. Place it directly over the wound and press hard enough to matter. If blood soaks through, do not peel the first layer off just to admire the damage. Add more material on top and keep pressing. Lifting the pad to check every few seconds is one of those mistakes people repeat because it feels active. It is not helpful.
Body position can help a little, though people make it mystical. If the person can lie down safely, that is often better than having them wobble around or sit bolt upright while losing blood. A calm flat position also helps if they are getting faint. But position is support work. Pressure is the main job.
The thing is, good bleeding control often looks boring from the outside. One person pressing steadily. Another calling for help, getting gear, watching the patient. Not flashy. Very effective.
Wound Packing Is Not Gentle Work
This is the part people avoid because it sounds rough. Fair enough. It is rough.
If a wound is deep, especially in an area where a tourniquet cannot be placed effectively, packing the wound with gauze can make the difference. You are not decorating the surface. You are filling the space where blood is pooling and pushing pressure down to the source as best you can.
That means taking gauze, ideally hemostatic gauze if you have it, and feeding it into the wound firmly, layer after layer, until the cavity is packed and you can hold direct pressure over the top. It is uncomfortable to think about and worse to do. Still, this is one of those cases where being squeamish helps nobody.
Plain rolled gauze works if that is what you have. Hemostatic gauze is better when used correctly because it supports clotting, but it does not replace pressure. People hear fancy product names and imagine magic. Not magic. Just better odds, maybe, when paired with proper technique.
And once the wound is packed, hold pressure. Don’t pack it and then fuss around reorganizing your bag like the important part is complete. It isn’t.
Tourniquets Deserve Less Myth and More Respect
A lot of bad thinking still floats around tourniquets. Some people are afraid to use them when they are clearly needed. Others act like slapping one on is the first answer to every bloody limb injury. Both instincts are sloppy in different directions.
A tourniquet is for severe life-threatening bleeding from an arm or leg when direct pressure is not enough, is not practical, or the scene is too chaotic to rely on hands alone. Massive bleeding. Amputation. Deep limb wounds that keep pouring despite real effort. That territory.
Place it high on the injured limb if you cannot clearly locate the wound in bad conditions, or two to three inches above the wound if the site is obvious and there is no joint in the way. Tighten it until the bleeding stops. Not until it feels snug. Not until the patient says wow. Until the bleeding stops.
That is where hesitation ruins things. An under-tightened tourniquet is miserable and ineffective, which is an awful combination. A properly applied one hurts. It is still the right move when the alternative is uncontrolled blood loss.
Write down the time if you can. Emergency crews need that information. Then leave the tourniquet alone unless a qualified professional takes over. This is not the moment for improvised adjustments because somebody nearby read half an article three years ago.
A Real-World Example People Remember
Picture a normal garage on a Saturday afternoon. Someone is cutting metal or wood, gets distracted for one second, and the tool bites deep into the forearm. At first there is disbelief more than panic. Then the floor starts getting spotted and the injured person says, a little too calmly, that it’s probably fine.
It may not be fine.
The useful responder in that moment does not deliver a speech. They get a cloth or trauma dressing on the wound and press hard. They tell someone else to call 911 now, not after a family debate. If the bleeding is soaking through and continuing fast, they expose enough of the arm to understand what they are dealing with. If direct pressure controls it, good, keep holding. If it does not, and the blood loss is still aggressive, the responder moves to a tourniquet on the limb and tightens until the bleeding actually stops.
What matters in that example is not perfect textbook posture. It is the absence of dithering. The body can survive a lot. It does not do well with delay while three adults negotiate whose idea sounds nicest.
That’s why I tell people to rehearse this mentally before they ever need it. Not because imagination saves lives by itself, but because familiarity cuts down on that stunned useless pause.
What an Everyday Bleeding Kit Should Have
You do not need a movie medic bag to handle the first several minutes well. You do need more than optimism.
A sensible bleeding kit is small:
- nitrile gloves
- compressed gauze or rolled gauze
- a pressure bandage or trauma dressing
- hemostatic gauze if you can afford and train with it
- a commercial tourniquet from a reputable brand
- trauma shears
- a marker to note tourniquet time
I would rather see a modest kit in three real locations, home, vehicle, and bag, than one elaborate kit sitting in a closet because it looked impressive when purchased.
And train with what you carry. Packaging matters. Stress matters. If you have never opened your gauze, never unfolded your tourniquet, never tried to apply pressure while your hands are slick or shaking a little, your equipment is partly theoretical.
The Patient Needs More Than the Wound Addressed
Once major bleeding is controlled or at least being actively managed, you start paying attention to the rest of the person again.
Keep them warm. Reassure them without lying. Watch for changes in alertness, breathing, skin color, and pulse if you know how. Do not give food or drink if emergency care is on the way and the situation is serious. Keep monitoring the wound, but do not keep disrupting your own work just because blood makes people anxious.
Shock is one of those words people toss around loosely. Real shock from blood loss is a body-wide failure in progress, not just feeling rattled. The person may look gray, act confused, get thirsty, become weak, or seem oddly detached. That’s the body’s supply lines starting to fail. At that point you are not just dealing with a cut anymore.
Even when the bleeding slows, stay humble. A person can crash later. Hidden injury exists. A soaked bandage with a now-quiet patient is not automatically a success story.
The Hard Part Is Decisiveness Without Panic
Good bleeding control has a certain personality to it. Firm, quick, not frantic.
That balance matters. Panic makes people skip steps or over-handle the wound. Timidity makes them press too softly and call it care. What you want is decisive pressure, clear escalation, and just enough calm to notice whether what you’re doing is working.
That is why I think bleeding control belongs near the top of practical preparedness. It is not exotic. It is not a wilderness fantasy skill. It shows up in kitchens, garages, roadsides, job sites, camps, and regular houses where somebody thought the sharp thing would stay predictable.
You may never need to use a tourniquet. Fine. I still want one nearby. You may never have to pack a wound. Good. I still want you to know what that means before the day arrives and your education is suddenly supposed to happen in real time.
Because when minutes matter, or really seconds at the start, the useful person is usually the one who understands that kindness and force are not opposites here. Sometimes the most caring thing in the room is a hard hand that does not let up.
Key Takeaways
- Severe bleeding becomes dangerous quickly and rewards fast, decisive action.
- Direct pressure only works if it is firm enough and sustained long enough.
- If blood soaks through, add material on top and keep pressing instead of removing the first layer.
- Deep wounds may need packing, and severe limb bleeding may require a tourniquet.
- A small real bleeding kit in the places you actually live and travel is better than a large theoretical kit.
Step-by-Step Preparedness Actions
- Build or refresh a bleeding kit for your home, vehicle, and everyday carry bag.
- Learn to recognize severe bleeding by speed, volume, and patient condition rather than drama alone.
- Practice opening gauze, pressure dressings, and your tourniquet before an emergency happens.
- Rehearse the sequence: gloves, expose, direct pressure, pack if needed, tourniquet if necessary, call for help.
- Keep the patient warm and monitored after bleeding is controlled or partially controlled.
- Replace used or expired bleeding-control supplies so your kit stays real, not decorative.
Quick Preparedness Checklist
- Nitrile gloves
- Compressed or rolled gauze
- Pressure bandage or trauma dressing
- Hemostatic gauze if available
- Commercial tourniquet
- Trauma shears
- Marker for tourniquet time
- Emergency phone access
- Basic training or rehearsal
Skills Practiced in This Module
- direct pressure
- wound assessment
- wound packing
- tourniquet application
- patient monitoring
- calm emergency response